
Most EBPs and published research were not designed or developed with input from BIPOC, Disabled, or Queer individuals, resulting in our approaches often perpetuating biases and reinforcing systemic inequalities, ultimately causing harm to marginalized communities. It’s a reality we cannot ignore, and the clock is ticking, my friends!
How Current Mainstream EBP Approaches Perpetuate Inequity + Injustice (Updated 2026)
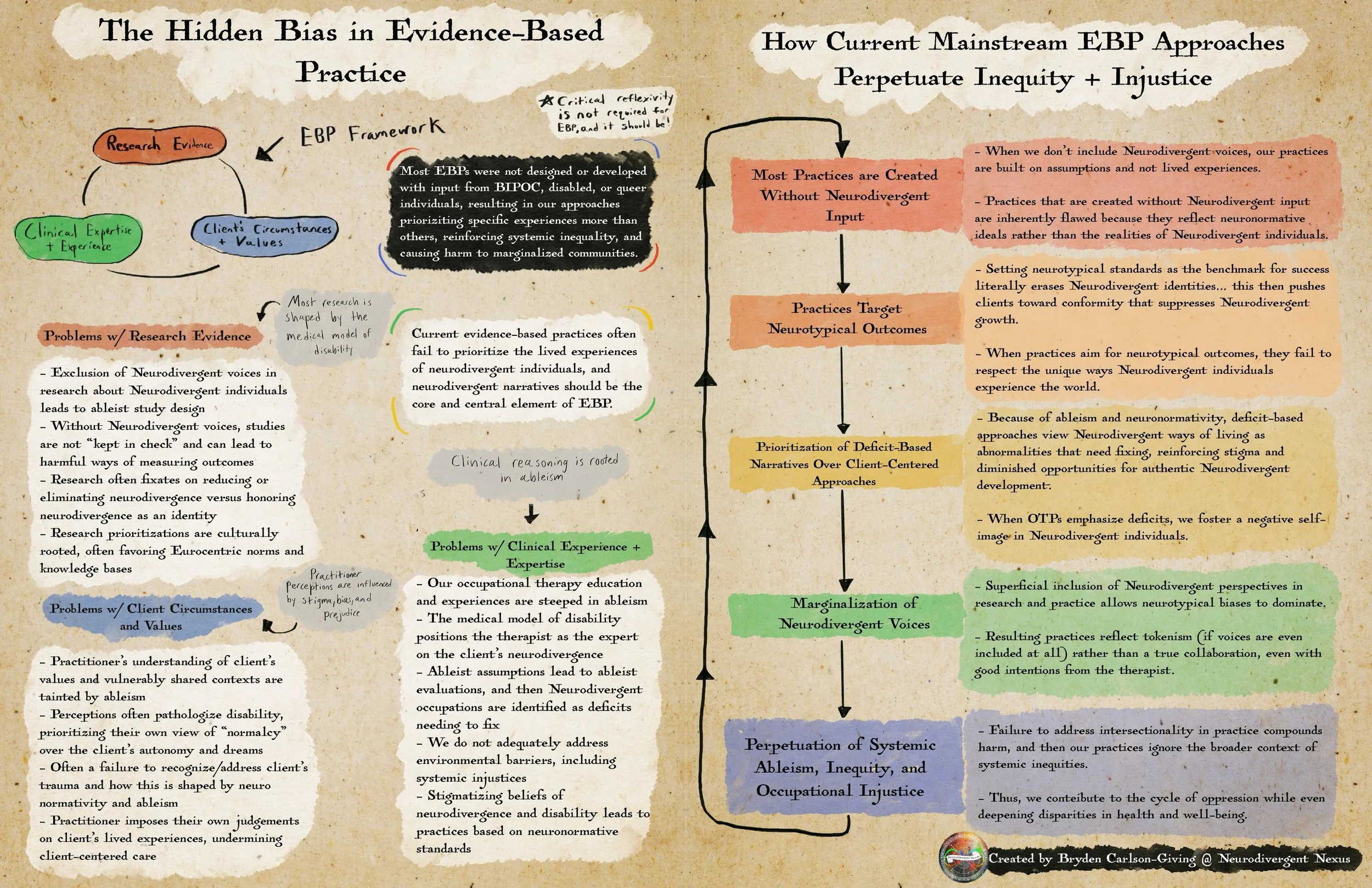
The Hidden Bias in Evidence-Based Practice (EBP)
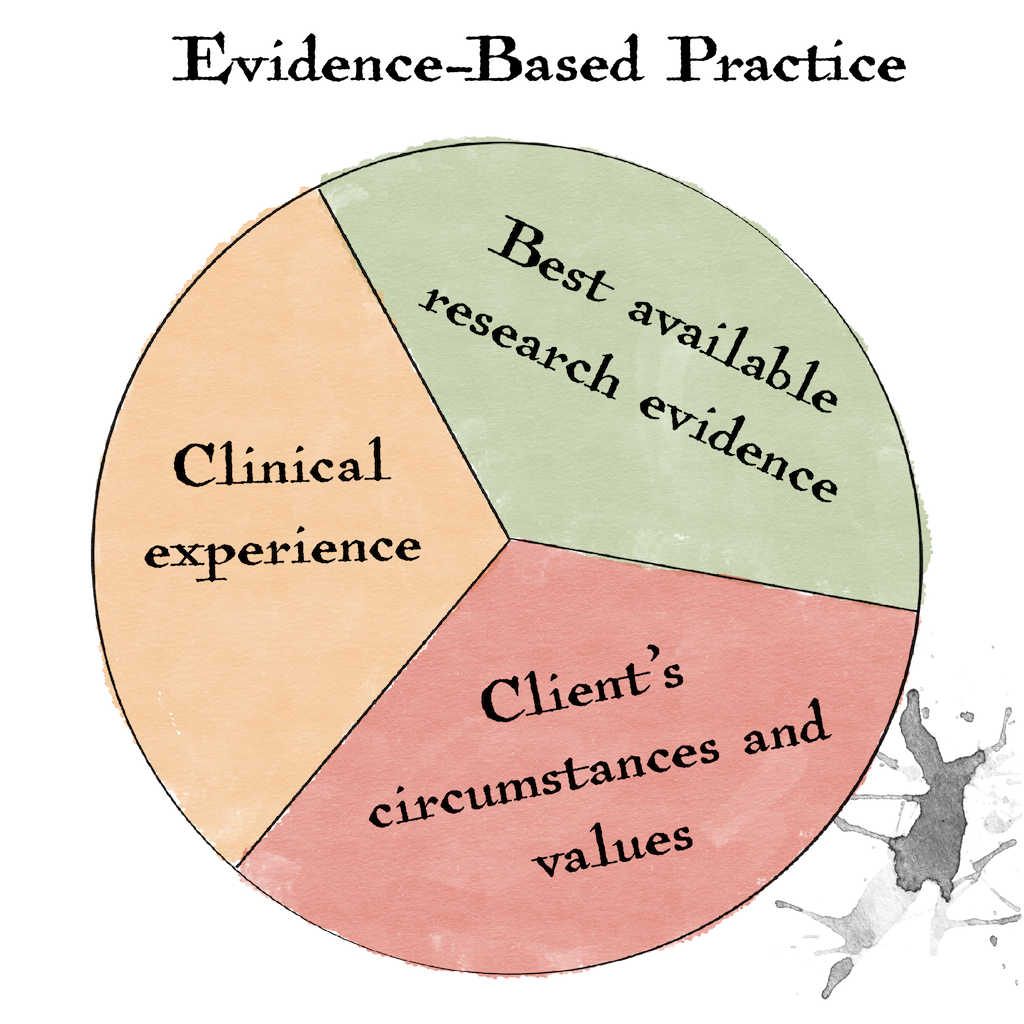
When an intervention is determined to be effective, who is the intervention actually effective for? Is it effective for the Neurodivergent individual based on their hopes, dreams, and input, or is it deemed effective by the non-Disabled researcher or practitioner based on what they assume to be important for the Disabled individual? What are the outcomes shared within the article, and who exactly is defining those outcomes? As shown in the illustration above, the issues with most EBP approaches extend beyond the research component and permeate the other two critical elements: clinical expertise and the client’s circumstances and values. Evidence-based practice has three components, including best research evidence, clinical expertise and experience, and the client’s unique circumstances. Current evidence-based practices often fail to prioritize the lived experiences of Neurodivergent individuals, and Neurodivergent narratives should be the core and central element of EBP.
Problems with Research Evidence (Most research is shaped by the medical model of disability)
There is an exclusion of Neurodivergent voices in research about Neurodivergent individuals, and this leads to ableist biases within the study’s design.
There is a significant absence of Neurodivergent lived experiences incorporated (authentically) within research.
Because of the absence of Neurodivergent voices, the designs are not “kept in check” and can lead to harmful ways of measuring outcomes (leading to the prioritization of neurotypical ways of living).
Research fixates on reducing or eliminating disability/neurodivergence vs honoring disability/neurodivergence as an identity that is valid and valuable.
Research methods and how we view which forms of knowledge are important are culturally rooted, prioritizing dominating Eurocentric and neurotypical culture within research.
Problems with Client Circumstances + Values (Practitioner perceptions are influenced by stigma, bias, and prejudice)
Practitioner's understanding of the client's values and vulnerably shared experiences are tainted by ableism.
Perceptions often pathologize disability, prioritizing their own view of "normalcy" over the client's autonomy and their hopes and dreams.
There often is a failure to recognize and address the client's trauma and how this is influenced by neuronormativity/ableism.
The practitioner imposes their own judgments on the client's lived experiences, which then undermines client-centered care (it is pretty impossible to provide client-centered care without addressing how ableism influences the practitioner and client relationship).
Problems with Clinical Experience + Expertise (Clinical reasoning rooted in ableism)
Our occupational therapy education and experiences are absolutely steeped in ableism.
The medical model of disability positions the practitioner as the expert on the client's neurodivergence.
Ableist assumptions lead to biased evaluations, where Neurodivergent occupations are identified and treated as deficits that need to be corrected because they deviate from what is considered the most “ideal” form of participation.
When our clinical reasoning is influenced by ableism, we often do not adequately consider how environmental factors (such as systemic injustices) influence participation.
Stigmatizing beliefs of neurodivergence and disability lead to practices based on neuronormative standards.
There is often a misinterpretation of the client's adaptive responses, and we reduce such responses as the client being "behavioral" versus doing the hard, inner work on how we and inequtiable systemic structures contribute to the adaptive responses.
How Current Mainstream EBP Approaches Perpetuate Inequity + Injustice
Incorporates a cycle of:
Most Practices are Created Without Neurodivergent Input -> When we don’t include Neurodivergent voices, our practices are built on assumptions and not lived experiences. Practices that are created without Neurodivergent input are inherently flawed because they reflect neuronormative ideals rather than the realities of Neurodivergent individuals.
Practices Target Neurotypical Outcomes -> Setting neurotypical standards as the benchmark for success literally erases Neurodivergent identities. This then pushes clients toward conformity that suppresses Neurodivergent growth (is it so terrible a thing to want to support Neurodivergent well-being?). When practices aim for neurotypical outcomes, they fail to respect the unique ways Neurodivergent individuals experience the world.
Prioritization of Deficit-Based Narratives Over Client-Centered Approaches -> Because of ableism and neuronormativity, deficit-based approaches view Neurodivergent ways of living as abnormalities that need fixing, reinforcing stigma and diminished opportunities for authentic Neurodivergent development. When OTPs emphasize deficits, we foster a negative self-image in Neurodivergent individuals. Remember, Neurodivergent individuals may want characteristics of their experience remediated, though if this is something we assume versus asking the individual, we amplify deficit-based narratives that are then ingrained within our clients.
Marginalization of Neurodivergent Voices -> Superficial inclusion of Neurodivergent perspectives in research and practice allows neurotypical biases to dominate. Resulting practices reflect tokenism (if voices are even included at all) rather than a true collaboration even with good intentions from the therapist.
Perpetuation of Systemic Ableism, Inequity, + Occupational Injustice -> Failure to address intersectionality in practice compounds harm, and then our practices ignore the broader context of systemic inequities, contributing to the cycle of oppression and even deepening disparities in health and well-being.
Given that many of our practices have ableist biases or exclude neurodivergent individuals from the research process, we must really think about and question the meaningfulness of our published research and the extent to which research influences our decisions.
References
Carlson-Giving, B. (2023). Embracing neurodivergent occupations and empowering disabled voices: A knowledge translation tool to support neurodiversity-affirming occupational therapy practice and challenge ableism within the profession. (Doctoral thesis). Boston University Research Repository. https://open.bu.edu/handle/2144/46622
Martinez, K., Callejas, L., & Hernandez, M. (2010). Community-defined evidence: A bottom-up behavioral health approach to measure what works in communities of color. Emotional & Behavioral Disorders in Youth, 11–16. https://www.engagelivinglab.org/wp-content/uploads/2021/04/Community-Defined-Evidence-Martinez-et-al-2010.pdf.
Tawa, K. (2020). Redefining evidence-based practices: Expanding our view of evidence. https://www.clasp.org/wp-content/uploads/2022/01/Evidence-Based-Practice-Brief_05152020.pdf
Wise, S. J. (2023). Lived experience informed practice: An alternative to evidence-based practice. https://medium.com/@livedexperienceeducator/lived-experience-informed-practice-an-alternative-to-evidence-based-practice-23a60e35602f